
Inflammatory Bowel Disease (IBD): Crohn's vs. Ulcerative Colitis
- Dr. Yusra Sharif

- Feb 21
- 3 min read
With Dr. Yusra Sharif — Gastroenterologist, Hadassah Hospital
Inflammatory Bowel Disease (IBD) is a chronic inflammatory disorder of the gastrointestinal tract and one of the most important high-yield topics for IMLE and USMLE preparation. Understanding IBD requires connecting pathophysiology, clinical presentation, colonoscopy findings, and treatment decisions — not just memorizing tables.
In this session, Dr. Yusra Sharif — Gastroenterologist at Hadassah Hospital — guides you through the essentials of IBD in a structured, exam-focused way.
Inside Brocali, this video is accompanied by summary pages, clinical reasoning breakdowns, and integrated exam-style questions to maximize retention and prepare you for rotations or licensing exams.
🎬 Watch the full video lesson here
What Is Inflammatory Bowel Disease (IBD)?
IBD refers to chronic inflammatory disorders of the GI tract, including:
Crohn’s disease
Ulcerative colitis
Both involve recurrent intestinal inflammation, leading to:
Diarrhea
Abdominal pain
Weight loss
Fatigue
IBD is complex because it combines immune dysregulation, genetics, and environmental triggers to create chronic inflammation.
Epidemiology, Etiology & Risk Factors
Feature | Ulcerative Colitis | Crohn’s Disease |
Age | 2nd–4th decades, 7th–9th decades | 2nd–4th decades, 7th–9th decades |
Race | Jewish > Non-Jewish white > Black > Latino > Asian | Jewish > Non-Jewish white > Black > Latino > Asian |
Gender ratio (F:M) | 0.51–1.58 | 0.34–1.65 |
Key point for exams: Crohn’s disease is slightly more common in males, UC slightly more in females, and both peak in young adults.
The exact cause of IBD is unknown. It results from genetic predisposition + environmental triggers + immune dysregulation + microbiota interactions.
Factor | Ulcerative Colitis | Crohn’s Disease |
Smoking | May prevent disease | May increase risk |
Oral contraceptives | No risk | Increased risk (HR 2.82) |
Appendectomy | Protective | Not protective |

Pathophysiology
IBD occurs when the immune system mistakenly attacks the gut lining.
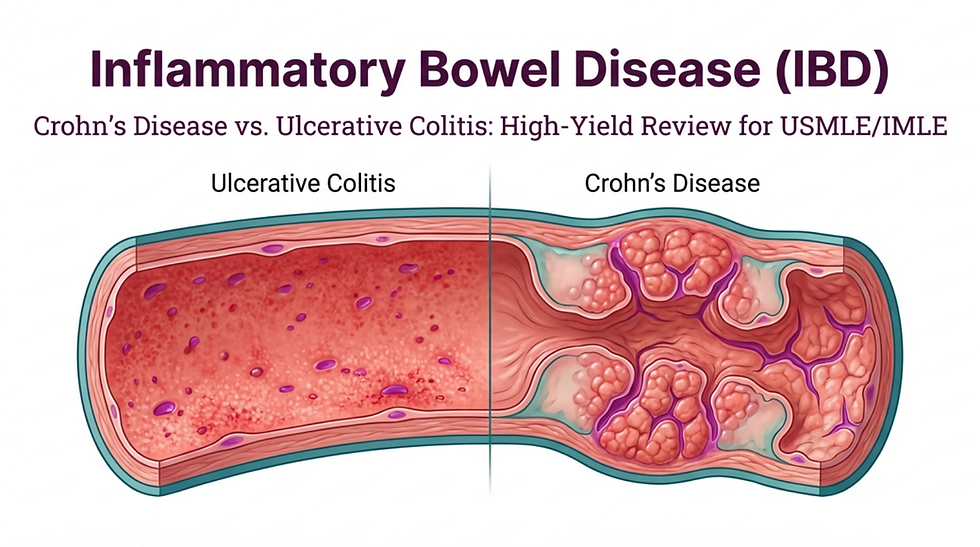
Crohn’s disease: Transmural inflammation → can affect any part of GI tract → thick bowel wall, skip lesions, fistulas, strictures.
Ulcerative colitis: Mucosal inflammation → continuous from rectum → thin bowel wall, pseudopolyps.
High-yield exam insight: Granulomas suggest Crohn’s; crypt abscesses suggest UC.
Clinical Features
Feature | Ulcerative Colitis | Crohn’s Disease |
Abdominal pain | Yes | Yes |
Diarrhea | Bloody with mucus | Chronic diarrhea |
Fever | Yes | Yes, high spiking if abscess |
Hematochezia | Common | Rare |
Tenesmus | Yes | No |
Perianal involvement | No | Common |
Strictures & fistulas | No | Yes |
Extraintestinal | Erythema nodosum, arthritis | Pyoderma gangrenosum, arthritis |
Note: B12 deficiency occurs with Crohn’s if terminal ileum is involved.


Diagnosis
Diagnosis relies on clinical features, colonoscopy, imaging, and histopathology.
Colonoscopy findings:
Crohn’s: Skip lesions, cobblestone mucosa, aphthous ulcers, strictures, fistulas
UC: Continuous mucosal inflammation, pseudopolyps, loss of haustra
Histopathology:
Crohn’s: Granulomas, transmural inflammation, deep ulcers
UC: Superficial mucosal inflammation, crypt abscesses, no granulomas
Imaging: CT/MRI enterography for bowel wall thickening, strictures, fistulas, abscesses
⚠️ Exam alert: Stool culture is essential to rule out infection before starting immunosuppressive therapy.

Management of IBD
Treatment goals: Reduce inflammation, induce remission, maintain remission, prevent complications
Therapy | Indications | Examples |
Amino-salicylates | Mild–moderate UC | Mesalamine, Sulfasalazine |
Corticosteroids | Moderate–severe flares | Prednisone, Budesonide |
Immunomodulators | Maintenance, steroid-resistant | Cyclosporine, 6-mercaptopurine |
Biologics | Moderate–severe, refractory | Infliximab, Adalimumab |
Surgery | Refractory disease, complications | Colectomy in UC, resection for Crohn’s strictures |
High-yield pearl: Crohn’s with fistula → first-line = Infliximab
Non-pharmacological: Nutritional support, smoking cessation (especially in Crohn’s)

Complications
Complication | Presentation | Management |
Toxic megacolon | Severe colonic distension, sepsis | Emergency surgery (colectomy) |
Strictures (Crohn’s) | Intestinal obstruction | Balloon dilation, surgery |
Fistulas | Perianal, enterocutaneous | Biologics, antibiotics, surgery if refractory |
Intra-abdominal abscess | Fever, leukocytosis | Drainage |
Colorectal cancer | Chronic inflammation | Screening colonoscopy every 2 years after 8 years |

How Brocali Teaches IBD Differently
With Brocali, you don’t just learn facts. You train your exam-thinking process:
Step-by-step video explanation
Summary pages for quick review
High-yield exam-style questions
Weak-point reinforcement
Integrated clinical reasoning
If you’re interested in seeing how Brocali works or have any questions about our learning platform, you can easily schedule a demo call at your convenience.



Comments